Overview
Avera Health, a leading healthcare system serving rural communities across the Upper Midwest, launched its innovative C-Airs program to revolutionize COPD care delivery in underserved areas. This groundbreaking initiative, supported by a substantial $1.2 million HRSA grant over four years (extending through August 31, 2027), represents a significant advancement in addressing the unique challenges faced by rural patients with chronic obstructive pulmonary disease.
The program provides hospital-level respiratory care services within the patient's home environment, offering a comfortable and familiar setting for recovery and ongoing management. This model seeks to improve access to specialized COPD care, enhance patient outcomes, reduce healthcare costs, and significantly decrease hospital readmissions. The program focuses on improving patient experience and outcomes, reducing hospital readmissions, enhancing access to care in rural areas, and streamlining care transitions. A key component of this initiative is the integration of Remote Patient Monitoring (RPM) solutions with an extended 90-day monitoring period, beginning with post-acute COPD patients.
The C-Airs program establishes a comprehensive care coordination network spanning three strategically located sites: Avera's Rural Healthcare division, Spencer Hospital, and Pipestone County Medical Center. This multi-site approach ensures broad geographic coverage while maintaining the personalized care that rural communities require.
Challenge
Traditional COPD care in rural settings faces several challenges, including limitations in specialist access, geographic barriers to care, potential for preventable exacerbations, and the growing need for patients to receive specialized respiratory care in their familiar home environment. Avera Health aimed to address these challenges by offering a safe and effective alternative for COPD patients requiring ongoing monitoring and support.
A critical aspect of this model was ensuring that patients at home received the necessary level of respiratory monitoring and education, comparable to what they would receive in a traditional clinical setting. This required a robust and user-friendly remote monitoring system to track respiratory parameters, facilitate communication with care teams, and ensure timely intervention if needed.
Rural COPD patients particularly struggle with access to pulmonary rehabilitation services, proper inhaler technique training, and consistent monitoring of their condition. The lack of immediate access to respiratory therapists and pulmonologists means that many patients experience preventable exacerbations that could be managed effectively with proper monitoring and early intervention.
Using tablets for video visits allows our Respiratory Therapy team to connect with high-risk COPD patients in a meaningful way.
Charlene Raley, Respiratory Therapist
Avera Health
Solution
To deliver specialized COPD care in rural home settings, Avera Health implemented a comprehensive RPM program with extended 90-day monitoring capabilities. This program utilizes the user-friendly cellular-connected tablets from Health Recovery Solutions (HRS) to bridge the digital divide for rural patients. Patients are equipped with Bluetooth-connected devices such as pulse oximeters, blood pressure cuffs, and scales, alongside digital spirometers, allowing for the continuous and remote monitoring of their respiratory and cardiovascular parameters.
The RPM platform enables the C-Airs care team to remotely monitor patient data, identify concerning trends, and intervene proactively if necessary. The platform allows nurses and respiratory therapists to utilize video functionality to connect with patients remotely, providing face-to-face interaction and personalized guidance on inhaler techniques, breathing exercises, and symptom management. The scalability of the solution also allows Avera providers the option to extend monitoring beyond the initial 90-day period, providing seamless continuity of care and supporting long-term patient well-being.
A critical innovation of the C-Airs program is its integration with existing care transitions teams, ensuring continuity between acute care and home-based monitoring. This collaborative approach maintains established relationships and protocols while extending the monitoring period significantly beyond traditional 30-day programs. The program incorporates comprehensive patient education, including proper inhaler technique training, COPD self-management strategies, and recognition of early warning signs.
Charlene Raley, Respiratory Therapist Coordinator at Avera, said about the program, “Using tablets for video visits allows our Respiratory Therapy team to connect with high-risk COPD patients in a meaningful way. We can see their home setup, walk them through troubleshooting equipment, and watch how they actually take their medications—rather than relying only on what’s documented in their chart. Watching patients demonstrate their medications and equipment helps ensure they are supported and confident, allowing us to trust that quality care continues at home.”
The program’s focus on patient identification and referral processes streamlines the transition from acute care to home-based monitoring, ensuring that eligible COPD patients are quickly enrolled and begin receiving enhanced support during the critical post-acute recovery phase.


Results
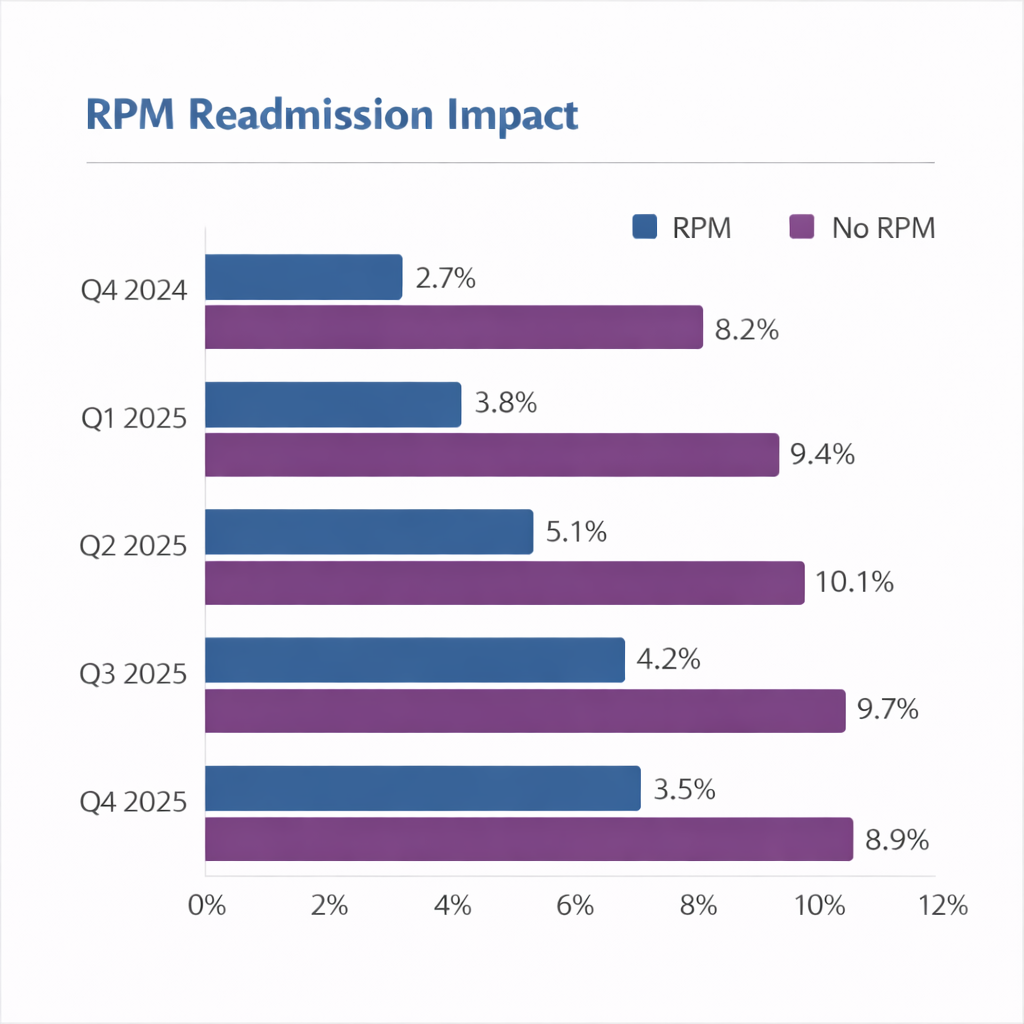
The integration of extended RPM into the Avera C-Airs program has yielded significant positive outcomes, demonstrating both efficiency and a tangible impact on rural COPD patient care. The program has shown remarkable success in reducing hospital readmissions, with RPM-monitored patients consistently experiencing readmission rates between 2.7% and 5.1%, compared to 8.2% to 10.1% for patients without RPM monitoring. This represents an average reduction of approximately 60% in readmission rates for COPD patients enrolled in the C-Airs RPM program.
The program has seen strong adoption across its three coordinated sites, with Rural Healthcare, Spencer Hospital, and Pipestone County Medical Center working seamlessly together to provide comprehensive care coverage. This multi-site approach has been particularly effective in reaching rural patients who previously had limited access to specialized respiratory care services.
A key focus of the program has been to increase the utilization of remote home monitoring for COPD patients, a goal that has been actively pursued and realized through the extended 90-day monitoring period. This represents a significant advancement over traditional 30-day monitoring programs, providing triple the standard monitoring duration during the critical post-acute phase when patients are most at risk for exacerbations and readmissions.
The C-Airs program has successfully demonstrated its ability to effectively manage COPD patients in their home environment while maintaining hospital-level oversight. The program's integration with existing care transitions teams has ensured smooth handoffs from acute care settings to home-based monitoring, maintaining continuity of care and established patient relationships.
The patient population benefiting from the C-Airs program encompasses post-acute COPD patients across rural communities, with particular emphasis on those at high risk for readmissions. The comprehensive approach includes not only remote monitoring but also extensive patient education covering inhaler techniques, breathing exercises, medication adherence, and early recognition of exacerbation symptoms.
Beyond the operational metrics, the implementation of the C-Airs program has contributed to improved patient education and engagement, fostering a better overall patient experience in rural settings. The program's structure and focus on proactive monitoring, combined with video-enabled consultations and comprehensive education, suggest a positive impact on reducing emergency visits and hospital readmissions while improving access to specialized COPD care in previously underserved rural areas.
The program's success in securing substantial HRSA funding and implementing coordinated care across multiple rural sites demonstrates its potential as a model for other healthcare systems facing similar challenges in chronic disease management and rural care access.